Why This Matters
Why early heart failure is often missed.
Heart failure is a hemodynamic disease that often develops before structural changes are visible. Traditional imaging tools may not detect disease early enough to intervene effectively.
- A normal echocardiogram does not rule out HFpEF.
- Standard resting echocardiography identifies only 34–60% of patients with HFpEF that was confirmed by invasive LVEDP testing.1
- Most HFpEF patients have normal or only mildly abnormal echo findings.
- Up to 68% of patients with confirmed HFpEF are classified as having normal or Grade 1 diastolic dysfunction on echocardiography, even when filling pressures are confirmed as elevated.2
- “Normal diastolic function” on echo often overlooks elevated filling pressures.
- Among HFpEF patients labeled as normal or mild diastolic dysfunction by echo, over 60% have elevated left-sided filling pressures when measured directly by catheterization highlighting false negatives from echo.2
This creates a critical gap precisely when early intervention can prevent progression.
How Vivio compares to other diagnostic modalities.
Diagnosing HFpEF remains challenging because accurately identifying elevated filling pressures is difficult without invasive testing.
While cardiac catheterization is the gold standard, non-invasive tools are more commonly used in clinical practice. However, no single non-invasive test has historically demonstrated both high sensitivity and high specificity.
Vivio changes that.
- Vivio detects elevated filling pressures with 80% sensitivity and 83% specificity validated head-to-head against invasive hemodynamic measurement, the gold standard physiologic evidence for heart failure diagnosis.3,4
- Non-invasive alternatives including echocardiography and BNP have well-documented limitations in reliably detecting elevated filling pressures and neither achieves both sensitivity and specificity above 70%.5
This balanced performance enables clinicians to detect heart failure earlier and with greater confidence, supporting more timely and appropriate treatment decisions.
Vivio is the only device available with sufficient sensitivity and specificity to drive a non-invasive diagnosis of heart failure


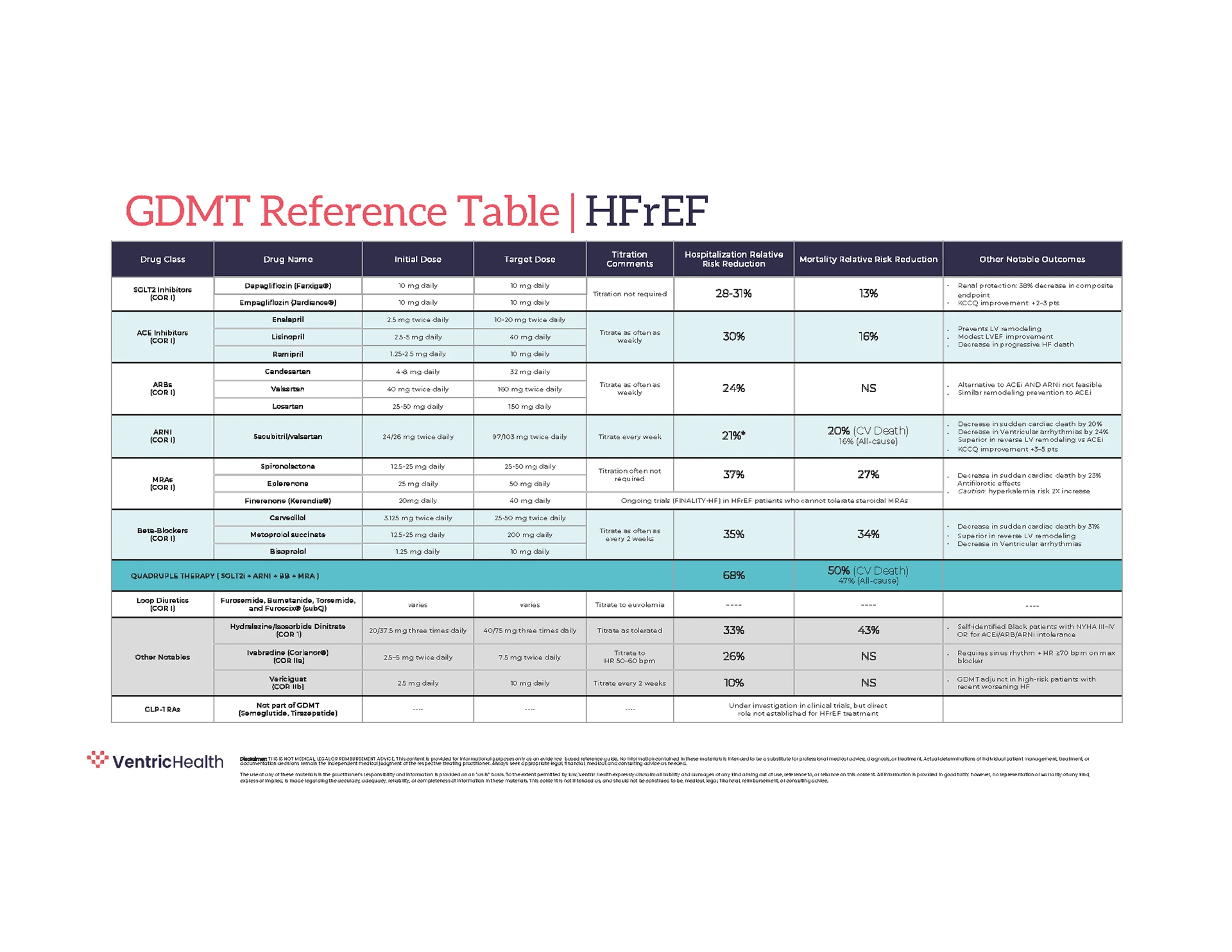
Clinical Framework
Vivio’s pathway to heart failure management.
Our workflow translates recommendations from the American College of Cardiology and the American Heart Association into a practical approach for identifying risk, confirming physiologic evidence, initiating Guideline-Directed Medical Therapy (GDMT) and monitoring patients over time. By aligning evaluation, diagnosis and management with established heart failure staging and treatment principles, clinicians can support earlier intervention, more consistent care decisions, and improved longitudinal outcomes.
A positive Vivio test is not the end of diagnosis. It’s the beginning of a structured, evidence-aligned care pathway.
Browse through each of the five pillars below.
Improving Care Decisions
Pairing Vivio with patient-reported outcomes.

Combining Vivio hemodynamic data with KCCQ symptom assessment enables:
- More precise staging of disease
- Better-informed treatment decisions
- Improved identification of patients needing escalation
This dual approach supports proactive, personalized care planning. See how Vivio incorporates the KCCQ, Kansas City Cardiomyopathy Questionnaire, directly into clinical workflows. Download our Pathway to Success Guide to learn more.
From Result to Action
What your Vivio test means.
Treatment decisions should align with both hemodynamic findings and symptom burden. Click on each stage below to explore recommendations and considerations for patient care.
Stage B Heart Failure
Clinical Profile: Elevated filling pressures without symptom burden
Stage C Heart Failure (NYHA Class I)
Clinical Profile: Elevated filling pressures with mild symptoms
Stage C Heart Failure (NYHA Class II)
Clinical Profile: Elevated filling pressures with moderate symptoms
Stage C/D Heart Failure (NYHA Class III–IV)
Clinical Profile: Elevated filling pressures with significant symptom burden
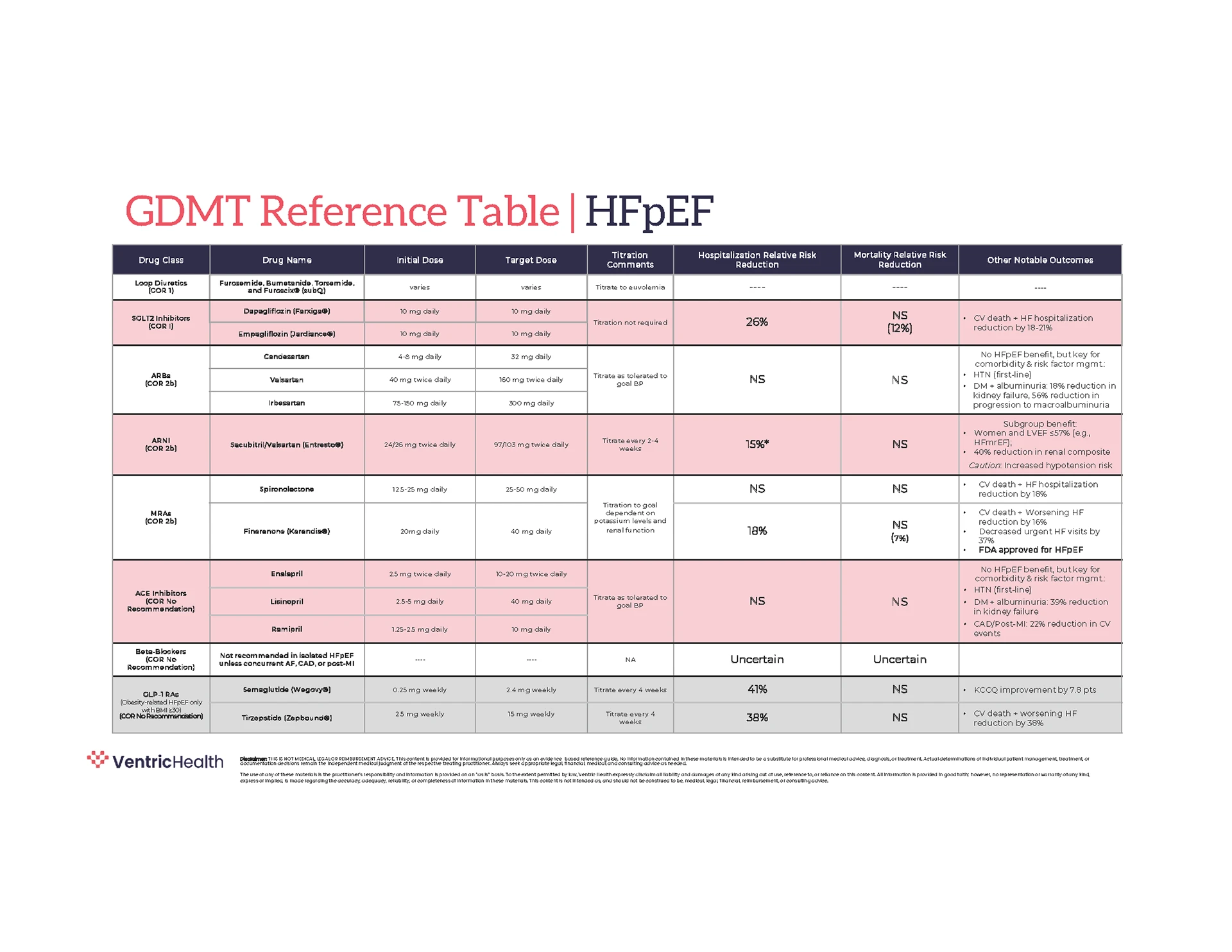
Guideline-aligned Care
Built on evidence-based heart failure management.
Treatment recommendations following a positive Vivio test align with established clinical guidelines.
When to Refer
Do all patients need an echo or cardiology referral?
Not necessarily. Early-stage patients can often be effectively managed in primary care using guideline-directed therapy.
Echocardiography:
- Recommended for patients with advanced symptoms (NYHA Class III/IV)
- Limited sensitivity in early-stage heart failure
- May not detect elevated filling pressures in early disease
Cardiology:
Most appropriate when:
- Symptoms progress despite therapy
- Advanced heart failure is suspected
- Additional diagnostic clarification is needed
Clinical Resources
Download practical tools to support heart failure management.